
Gracey's, Gracey's, Gracey's Galore
The Gracey series is a must-have in any hygiene tool kit. One challenge with Gracey’s is that they are a challenge to sharpen. The exciting news is that American Eagle Instruments have made it so you no longer have to worry about sharpening them anymore, by manufacturing them with the XP Shapren-Free Technology. When using any instrument with XP Sharpen-Free technology be sure to:
NOT sharpen them
Use a modified exploratory-like stroke to remove deposits (see videos below for demonstration)
Not to “pop” of the calculus, but to shave it off from the top of the deposit to the tooth, similar to how it is done with an ultrasonic.
Check out the 15-16 or M, L, and B surfaces and the 13-14 for D surfaces below
15-16 Gracey
13-14 Gracey with XP Sharpen-Free Technology
Double Graceys are also made with XP Sharpen-Free technology. A double Gracey is a combined 11-12, 13-14 into one. You no longer have to pick up two different Gracey instruments during treatment or figure out how to sharpen such an intricate instrument.
BEST. THING, EVER. INVENTED!!!
Check out the posterior and anterior double Gracey instruments in our latest videos below.
Double Gracey Mini anterior and posterior
Double Gracey Standard anterior and posterior
At the recent American Dental Hygienists’ Association Annual Session, a lecture was provided by Anna Pattison, an instrumentation guru. Our own Jessica Atkinson was able to attend and learned to take shorter strokes, at a rolled adaptation interproximal to reduce burnishing calculus. You can see this adaptation stroke in the videos above.
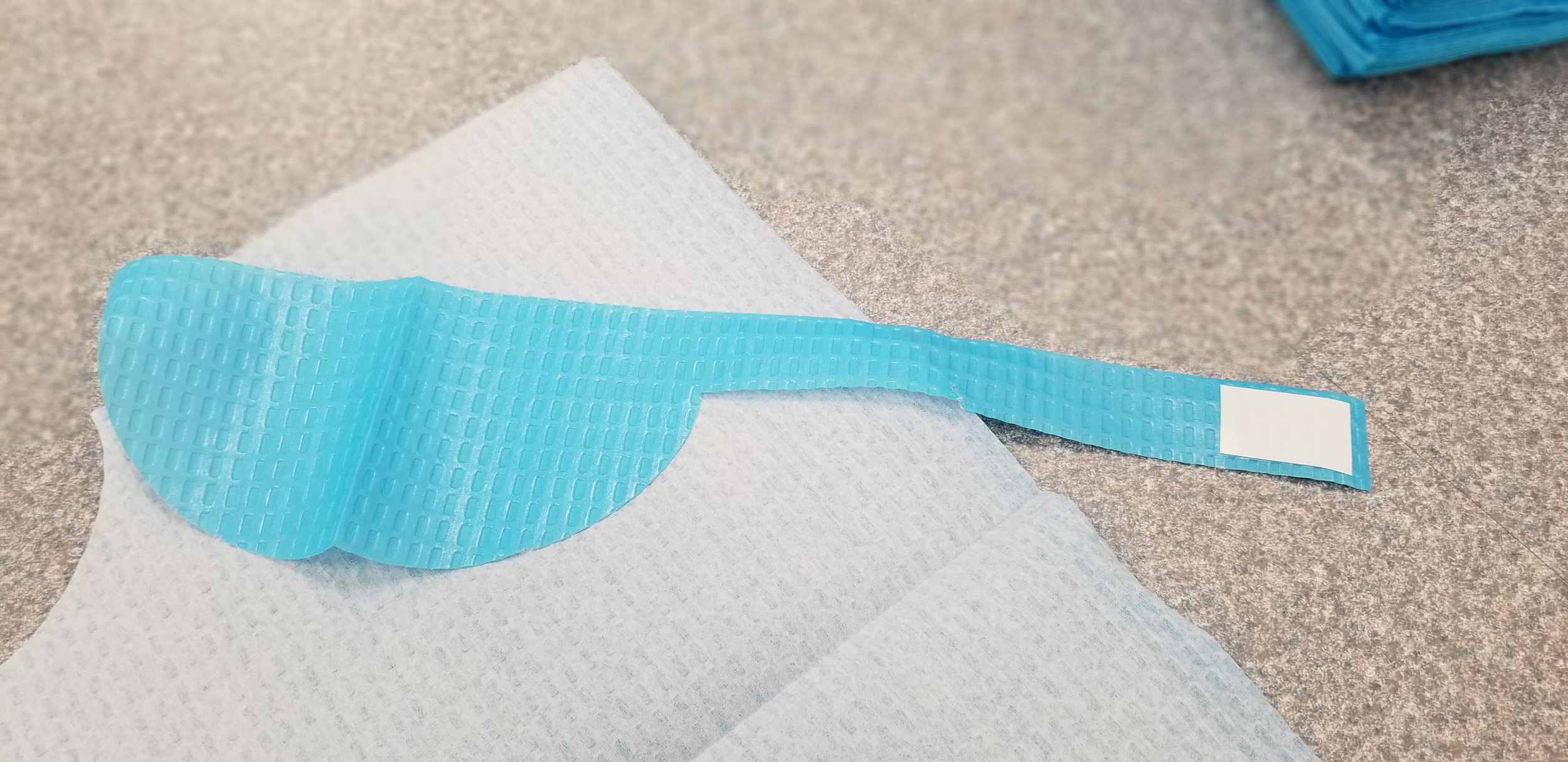
The TapKin A Bib Clip Free Patient Cover
As dental hygienists one of our biggest rolls is that of the infection control guru in the office. I would dare say that we are the most knowledgeable on this topic in the office. Being a dental assistant prior to becoming a dental hygienist, I can say that as dental assistant I lacked the knowledge of the importance of proper infection control. In dentistry we are always searching for ways to reduce cross contamination and at the same time increase efficiency. Check out our latest video below and learn all about the TapKin, a bib clip free patient cover, that allows you to #ditchthebibclip and reduce cross contamination.
We are giving away a box of TapKins on our Instagram @hygieneedge! Head over there to enter to win!
If you just want it now TapKin is offering a 5% off discount to all of our viewers, enter “EDGE” at checkout on the TapKin website. The discount code will be active until August 1st, 2019.
Contest rules can be found HERE.
New RDH Grad Advice

Congratulations to all the amazing new 2019 dental hygiene grads! As we all know, hygiene school is hard, fun, stressful, empowering, all the emotions wrapped up in a 2 year package. Graduating and passing boards exams are such a highlight of the entire experience. I’m not going to lie- I have some of the best memories of college in my last semester of dental hygiene school. Possibly because the lows are very low, but the highs are high?
And now- it’s over! Congrats again. But, now what? Transitioning from being a (more than) full time student to looking for the perfect office to call home can be tricky. We’ve asked dental hygienists from all over the country to give their advice. Here are some of our favorites:
“Take it one day at a time. Don’t let one bad day, one bad appointment, one bad set of radiographs sully your entire career”
“Stay at an office for at least 2 months before jumping ship-unless it’s a horrible situation”
“Be a member and stay active in your professional organization, the American Dental Hygienists’ Association. You never know who you will meet through the association, or where your career will take you. Having a backing as well to support the profession as you grow into it is also amazing.”
“Invest in yourself from day one. Buy your own loupes and saddle chair if you need to. Take time to stretch during the day. Taking care of yourself should be #1. Isn’t there a saying that you have to take care of yourself before you take care of other people?”
“Be a life long learner. Dentistry is a science, and it’s always changing and improving. Stay up on your CE credits and classes not because you have to for your license, but because you want what’s best for yourself and for your patients.”
What’s your advice for a new grad? Or the best piece of advice you received as a new graduate?
April Hygiene Round Up
April’s Round Up of some of our favorite dental posts, articles, and products.

It’s Spring! So much energy comes with spring and we love the feel that comes with the season’s change. The shift as well definitely renews our love for our amazing profession and learning! Here are a few things we’ve been looking at and thinking about this month. What have you been focusing on this Spring?
April is National Oral Cancer Awareness Month. Do you do anything to celebrate with your office or community?
The Dental Herb Company has created a new gum at home treatment for perio patients called PerioSpot. Gel can be directly placed on problem areas for patients. Using the same essential oils as they use in the popular Tooth & Gums Tonic, the theory is to decrease inflammation.
We are speaking at an upcoming Utah Dental Hygienists’ Association Central Component Meeting on May 4th. We’d love to have you there! Register today to save your spot.
We also just booked our tickets to the ADHA Convention in Louisville! Who else will be there?
Would you wear a long sleeved scrub top to do hygiene in?
Do you worry about W2s or 1099s when you temp?
What RDH's Are Talking About: Colgate SF

Colgate total: Old formula and packaging and New SF formula
A few months ago, Colgate released a new formula for their Colgate Total toothpaste. The triclosan was pulled, sodium fluoride was added as the active ingredient, and the name was changed to Colgate Total SF.
What is Triclosan?
Triclosan has been around since the 1960s as a pesticide, but has found its way into shampoos, hand and body washes, and toothpastes in the last few decades. Colgate has been using Triclosan in their Colgate Total Toothpaste for years. It has been shown to be antibacterial and can decrease smells.
Why was it removed?
The downside with triclosan is the wide range of antibacterial effects. Because of this, some researchers are worried about overusing triclosan, creating resistant and harder to kill bacteria. Also, it could be getting into the water and affecting aquatic life.
There currently has not been any research that triclosan in your toothpaste will hurt you or be a problem in the short term. There is some early research, however, suggesting long term use may affect hormones, prompt cancer cells, and make it easier for antibiotic-resistant bacteria grow (like MRSA). Most studies are only done on cells or animals, so it’s not clear if humans will have an effect from triclosan.
Either way- if triclosan is harmful or not- it has been pulled from Colgate’s most popular, and one of my personal favorite, toothpastes. The tricky part of the change is it has changed the flavor and the texture of the toothpaste slightly. You may have patients mention they notice a difference and, honestly, may not like the new formula, especially if they have been a long time Colgate user. Just as when Crest ProHealth was released, there were definitely some resistance to that as well. Even from me! I didn’t love the Pro Health taste, the gritty texture, or even the new flavor. However, after a few runs with the new formula, it has definitely improved over the years. I’m thinking that Colgate Total will be the same- some heartache at first from consumers, but they’ll come around with some time.
What are your experience been with the new Colgate Total SF?
Have you had patients mention they’ve tried it or asked you questions about it?
Celebrate Children's Oral Health Month

It’s February! It may be more than half over, but there’s still time to celebrate National Children’s Oral Health Month with your own kids, your patients, your neighbors, your online friends, or whoever!
Oral health in children has become a passion of mine since last year. I’m not going to lie. I was never a fan of treating kids in the dental office. The appointment is always rushed, stressful, the kids are wiggly, and teaching them seemed silly as all they wanted to talk about was their new toy or what show they liked to watch. I even have a 4 year old, but those pedo appointments always made me nervous. However, last year, our family were able to take care of 2 little girls (4 & 3 years old) for a few months. Having them in our home showed how important my role of a dental hygienist is to the oral health education of kids. They had been going to the dentist every 6 months through a school program, but hadn’t been receiving the education about oral health at home. They didn’t own toothbrushes, loves to snack on carbs all day, and unfortunately had decay on every tooth. This inspired me to be the best hygienist for these patients! They are so little, so cute, so willing to learn, and so quick to pick up on what’s being taught! Even though they may not be getting as much support at home that I’d like to see, we can show a lot of love and teaching at each appointment to make the dental office a positive, lifelong experience.
So, let’s not be nervous about seeing pedo patients, but let’s celebrate them this February with National Children’s Oral Health Month!
Looking for some ways to celebrate? We rounded up a few of our favorite crafts, teaching aids, and activities to highlight the importance of oral health.
The ADHA and the American Academy of Pediatrics have worked together this year to create a campaign and educational materials about the importance of oral health for moms and their babies. Let’s keep those teeth healthy from day one!
ADA National Children’s Dental Health Month
The ADA has created 2019 posters to help promote this year’s NCDHM, as well as helpful information about press releases, etc to help you promote the month in your neighborhood or city. There are fun worksheets as well in both English and Spanish to not only use this month, but anytime!
This download looks really cute! Full of ideas, printables, and and activities to use this month, but could be used at any school visit throughout the year.
Colgate Bright Smiles, Bright Futures
Colgate is dedicated to helping kids. Through the Bright Smiles, Bright Future website, you can request the Colgate Mobile Dental Clinic Van to visit a site, or find some videos that could be shared on your Facebook Page to promote this amazing month of health.
Why not try an experiment at your office or with your kids to show the importance of good home care and the negative effects of soda on teeth.
What do you do for National Children’s Dental Health Month?
Five Characteristics of a Profitable Dental Hygiene Department
Our latest article is brought to you by Speareducation.com. They are an amazing resource for dental teams to learn about all thing dental. Be sure to check them out at Speareducation.com.
Five Characteristics of a Profitable Dental Hygiene Department
Every progressive and profitable dental hygiene department has these five characteristics in common: solid clinical protocols, statistics and benchmarks, appropriate service mix, confident communication skills and "A-Team" hygienists I will discuss all five in this article.
Solid clinical protocols
Having solid evidence-based clinical protocols for each hygiene procedure is the cornerstone of a progressive and profitable hygiene department. It’s essential that these protocols are agreed upon and understood by every team member. The doctor(s), as well as the hygiene team, must recognize disease in its earliest stages and diagnose active infection with the same parameters. AAP case typing should be applied to each perio patient and treatment planning for treating periodontal disease follows agreed upon prescribed protocols and parameters.
See an example of what your clinical protocols for a preventive prophy might include below. As you read these protocols, keep in mind the ADA 1110 descriptor states following: Removal of plaque, calculus and stains from the tooth structures in the permanent and transitional dentition. It is intended to control local irritational factors.
Solid clinical protocol for 1110
Health history and risk factor assessment, every visit
Blood pressure screening, every visit
Current radiographs showing alveolar bone, when necessary
Head and neck exam/oral cancer screening, including the use of visual enhancement technology if available, once per year
Restorative evaluation and discussion, including pending and new treatment options, using an intra-oral camera and caries detection device if available, every visit
Periodontal screening, every visit (unless providing a comp perio evaluation)
Spot check: record pockets and bleeding only
Comprehensive periodontal evaluation at least once per year regardless of case type, which includes:
Six-point/tooth pocket measurement
Bleeding sites
Pus
Furcation
Mobility
Recession
Clinical attachment loss
Tissue response
Personalized patient education and treatment planning when disease activity is present
Personalized home care products and techniques, every visit
Personalized adjunctive therapies as needed:
Flouride
Sealants
Treatment rinses
Whitening gel
Specialty procedures
Personalized recall interval, every visit
While these clinical protocols serve as a guideline for every prophy appointment, as clinicians we understand that we must use our clinical care skill and judgment with each patient to customize the appointment and manage our time. The patients’ priorities, chief concerns and needs always come first.
Statistics and benchmarks
In a lot of ways, this is a misunderstood topic. Often, when the topic of statistics comes up, hygienists react adversely, because we immediately think production. While production is a part of the equation in a dental hygiene department, it’s actually so much more! Tracking performance statistics, that is how much of each procedure you perform, can tell you a lot about your overarching treatment philosophy and clinical parameters.
Let's look at a few examples from profitable dental hygiene departments:
An office in California, with three doctors and five hygienists were providing periodontal procedures at 21 percent. A perio percentage of 21 percent might appear high, but in this case, it primarily represented patients in maintenance, rather than active treatment. During coaching, this office discussed what they believed about treating periodontal disease, and guess what they discovered? They weren’t walking their talk. After they tuned up their solid evidence-based clinical protocols their perio increased to 31 percent. They experienced a 64 percent increase in periodontal infections treated with non-surgical therapy. (4341/2) This shift came as a result of identifying a lack of clinical continuity, which was revealed in this practices statistics and benchmarks.
I’d like to share two more examples of how statistics and benchmarks can confirm that each hygienist is ‘living’ the treatment philosophy and clinical parameters of a profitable dental hygiene department.
Brooke is a member of a five-doctor practice and one of eight hygienists in this busy Alabama office. In just three short months, she raised her personal perio percentage to 31 percent. She is spending 31 percent of her time providing periodontal care for her patients. This is also reflected in her production, which has increased by $120/day!
Let’s look at another example.
Kristy, one of five hygienists in a three-doctor Arizona practice, a full year following initial training, is maintaining a perio percentage of 36 percent, with an average hourly production of $222, up $92 from her beginning production per hour.
It’s clear from these statistics that these ladies are ‘living’ their treatment philosophies and making sure that the patients in their care are receiving periodontal therapy when it’s needed. And the fact that their dental hygiene departments are profitable proves that they are providing a high level of service and professional care for their patients. If you haven’t already done so, setting some reasonable and clear goals for the dental hygiene department provides benchmarks for performance so that each Hygienist can measure their progress and success. Below you will find the current industry standards. Use these guidelines to help set your goals.
Hygiene industry standards:
Perio percentage 35-40 percent
Open time percentage 8-10 percent
Hygiene production 3x salary + benefits
Prophy (1110) to perio maintenance (4910) ratio of 3:1
Balanced service mix
Balanced service mix is a reflection of your clinical philosophy. Looking at service mix is essentially looking at the variety of services, beyond a basic prophy, that are being offered and delivered in your dental hygiene department.
There really are no industry standards for dental hygiene department service mix, which makes this statistic driven completely by philosophy and protocol. I’d like to make the assumption that if you are reading this article, you have also watched the Principle-Based Dental Hygiene course available through Spear’s Course Library in the Staff Training section. Your principles of care will drive your service mix.
For example, if one of your principles includes eliminating sub-gingival bacteria, then your statistics would reveal the regular use of a locally applied antibiotic (LAA) such as Arestin. Typically, I would expect to see at least one site of LAA per quad of therapy (4341/2) and at least 30 percent of periodontal maintenance patients’ receiving one, two or three sites of LAA.
Additionally, if you believe that adult fluoride application can lower caries rates, decrease root sensitivity for those with recession and help your patients protect their investment in restorative dentistry, then your statistics would reflect the regular application of adult fluoride varnish. For an office that has adopted this philosophy I would expect at least 50 percent of adult patients would be receiving fluoride. To achieve that percentage, all adults would have to be offered the opportunity to take advantage of a fluoride varnish application.
Radiographs are another area you should evaluate. What is the frequency of PANOs and FMX being sourced from your dental hygiene department? Visualizing alveolar bone is a key component of periodontal diagnosis and risk evaluation for future periodontal disease. The use of seven Vertical BWs rather than four Horizontal BWs can help you visualize all areas of alveolar bone. When radiographs are neglected, disease will be missed.
Time management and communication skills
At the dental hygiene chair we walk a tightrope between data collection, delivery of care and education/enrollment. We must make the most of the precious 60 minutes we have with each patient. The first step in this process is chart review!
You must know the following, before seating your perio maintenance or recall patient, to make a realistic plan for today’s dental hygiene appointment:
Previously reported risk factors, health history concerns, medications etc.
Incomplete diagnosed treatment of any kind
Periodontal case type
Radiographic needs
Once the patient is seated, break the dental hygiene appointment down into three components, as we do at Inspired Hygiene:
20 minutes – Data collection/patient education
20 minutes – Patient education/clinical procedure
20 minutes – Clinical procedure/doctor exam/documentation
It’s always best to provide a periodontal screening, rather than a comprehensive perio exam when radiographs and doctor exam are scheduled to facilitate time management. In addition, the doctor exam should occur in the second 20 minute time frame whenever possible. This will prevent the hygienist from having to wait on the doctor and increase case acceptance measurably.
Using words and phrases that have the biggest impact can help you get your point across quickly. A great exercise you can do as a team is "Start Saying/Stop Saying." I’ll get you started; see how many more words/phrases you can come up with!
Stop saying:
I found ...
You need ...
Inflammation ...
Little ...
Start saying
Bob, you have ...
Sue, it’s in your best interest ...
Infection ...
Slight, moderate, severe ...
“A-Team” Hygiene Department
Having solid clinical protocols in place is half the battle. Having the correct team members in place is the other half. All too often I find myself in a discussion with a client that involves an underperforming or negative hygienist. And after some coaching to help this team member things get better for a few weeks or even a few months. Soon, however, we are having the same discussion about the same team member again, and again. Does this sound familiar? If so, it may be time to ask yourself if you have the right players on your team.
Dental hygienists are well-paid, highly trained and skilled, health care professionals and should conduct themselves as such. An A-Team hygiene department consists of those that exhibit strong levels of commitment and dedication to not only their patients, but their team members as well. An A-Team hygienist may emerge as a leader; you will recognize them by their qualities and behaviors:
On time and prepared for the morning huddle by having reviewed each patients’ chart and treatment needs
Timely with patient appointments
Compassionate with patients and team members
Mastered the art of a great handoff
Participates actively in a positive encouraging way during team meetings
Has a generally positive outlook with a ‘can do’ attitude
Willing to try something new if it’s better for the patient and the business
When faced with a challenge will often come up with a solution
Puts effort into using correct verbal skills and values communication
Willing to grow and develop (with) the hygiene department
Understands the business of dental hygiene and the importance of tracking statistics
Seeks out advanced continuing education, rather than just fulfilling the minimum requirements
Having a solid foundation with clear systems, written protocols and agreements in place creates an environment, and the opportunity, for hygienists to function at the top of their game. Setting some reasonable and clear goals provides benchmarks for performance so that each hygienist can measure their progress and success. A-Team hygienists can be developed when these systems are in place.
Kim Miller, RDH, BSDH, is a contributing author for Spear Education.
A 10-Step Occlusion Checklist for the Hygiene Room
Have you heard of speareducation.com. They are a wonderful resource for any office seeking to continually build their team. They have lots of great content. Our latest article is brought to you by Speareducation.com.
______________________________________________________________________________
A 10-Step Occlusion Checklist for the Hygiene Room
The hygiene visit is a cornerstone in a busy general dental practice. It is where patients not only receive education and treatment, but also receive an examination of the oral soft tissue structures, the dentition status and the periodontal health. Each status is documented in detail and a history is created so it can be followed over time. Often an initial diagnosis and additional treatment recommendations also begin in the hygiene room appointment.

To achieve all of that in one very full appointment requires streamlined systems to maximize the productivity. The periodontal and dentition documentation are well established for the hygiene appointment. Probing depths and bleeding indexes, tooth numbers and restorative tracking are ingrained early in education and in clinical practice. What is less systematized is tracking the developing occlusion.
An important aspect of treatment decisions is using the patient history to understand the progress or severity of problems, using that to guide recommendations. Equally valuable is monitoring the patterns that are expressed in dental, jaw and facial development. Using a checklist system will help to identify issues we don’t always see if we don’t look for them. When it comes time to make a treatment referral it is beneficial to know when the cross bite developed. Or that the open bite has reduced with each six-month exam. Your treatment decisions may alter if the airway has not improved for the last two visits. Or if the midline is now off by another millimeter. With good documentation you are able to inform patients and families of issues that may need additional evaluation in the future. It will not be a surprise when you make a referral for an issue that you have already identified for them.
Using this “top 10” checklist can organize your documentation into an easy system to follow and update with future visits. As with any new system, it will take several times to become efficient, but once practiced can be completed in a few minutes.
Some considerations are listed below for each measurement.
The Checklist
1. Overbite: A deep bite can be associated with incisor wear. An open bite may have a habit or airway component.
2. Overjet: An excess can indicate a developing Class II growth pattern, dental protrusion or narrow arch width.
3. Upper midline: With lips at rest and slightly apart, midline should be within the philtrum (cupids bow). Off-center midline can indicate crowding, a developing crossbite with palatal incisor eruption, or early primary tooth loss.
4. Lower midline: This can be an indication of a lower jaw growth asymmetry, crossbite, early loss of primary teeth or crowding
5. Cross bite: Posterior can indicate a lower jaw growth asymmetry or a narrow upper arch; anterior can indicate a developing Class III pattern or crowding with palatal eruption and a functional shift.
6. Crowding: Mild is in the range of up to 4 mm of crowding, moderate range 6-8 mm or more, and severe is 8 mm of crowding or more.
7. Palate width: 36-38 mm is the range of normal with normal range tooth size. Less than 31 mm and there is a high risk for severe crowding.
8. Canine position: Screening for canine position by age 10 can increase the potential to successfully improve an ectopic (impacted) eruption pathway. Comparing the angle of the canine crown to the distal contour of the lateral incisor from crown to root tip can indicate if active treatment is indicated.
9. Missing teeth: Noting this early can assist with awareness and planning discussions for replacement.
10. Airway: Easy breathing through the nose with lips resting together is ideal. Stuffiness, tonsils and adenoids, allergies, lip strain and snoring can be indicators for referral to an ENT for evaluation.
Donna J. Stenberg D.D.S., M.S., P.A., Spear Visiting Faculty and Contributing Author. djstenbergdds@gmail.com
References
McNamara JA, Brudon WL, Kokich VG. Orthodontics and Dentofacial Orthopedics. Ann Arbor, MI: Needham Press; 2001.
Schindel RH, Sheinis MR. Prediction of maxillary lateral-incisor root resorption using sector analysis of potentially impacted canines. Journal of Clinical Orthodontics. 2013;47(8):490-493.
Turning My Restorative WREB "Failure" into a "Success"
Thank you Nancy Huckvale for writing and being honest about your WREB experience! Nancy is an amazing dental hygienist who is dedicated to her patients and her family.

To my dental hygiene lovelies,
After graduating dental hygiene school and spending my first year in my home state of Utah, I moved up to the beautiful area near Vancouver, Washington. This move started me on a confusing process of applying for my WA license where somehow I ended up with an incorrect understanding that it would be REQUIRED for me to have a restorative license, along with a general dental hygiene license, if I wanted to work in WA. So I signed up for an expanded functions restorative class and the fun began! *Insert a waa-haa-haaaaaa sound in the background here*
The truth was, however, because I already had my hours built up from my time working in Utah, I didn't need any additional classes or tests beyond what I'd needed to get my UT license. I didn't learn this until after I had failed the restorative WREB test three times. I didn't learn this until after I had spent over $6,000 (yes, six-freakin'-thousand dollars) invested into taking necessary classes, books, hotel/gas fees to travel to take the tests, remediation classes, etc later. I didn't learn this until I had shed many heart-broken tears of feeling like I myself was a failure to match the word "FAIL" that came back on each of those test results.
After learning that I didn't actually NEED to take that horrible, awful test again, I had a choice. I got to make the choice of keeping my 'limited hygiene license' forever (easier, less expensive, 'safer' choice) or paying another $600 and giving myself one last chance just for the heck of it. Taking this test simply to prove to myself I could do it. (exciting, more expensive, challenging, Ninja choice.) You can guess what choice I made!
Learning how to do fillings came so un-naturally to me. It felt so... awkward. The physical piece of dentistry in general seemed to come un-naturally to me. In dental hygiene school I struggled to feel the calculus with the explorer, let alone remove it with scalers. I didn't feel like "I've got the hang of this teeth- cleaning thing!" till probably about six years after graduating and working in the field. I love people, and I love science. So the social/human interaction and relationship piece of dentistry comes natural, and understanding the biology and chemistry behind dentistry makes sense in my mind. But the ARTISTIC piece I've had to invest much energy into developing. That part of being able to see the anatomy of the teeth as ART while you're creating, seeing angles while giving injections, building a detailed filling, or removing stains during a prophy-- that cool creative, art-sy piece! This would be confirmed in the example of what I see vs. what my art-sy, creative (hunk-y) husband sees when we each looked at a big blank wall in our home. I simply saw a big blank wall complete with crickets chirping in the background, while he was looking at a canvas to work magic on and already had 10 ideas of different ways we could create in that space!
I spent hours and hours learning and practicing fillings by watching YouTube videos, reading and highlighting books, observing hygienists and dentists in the operatory doing fillings, asking questions, sitting at home in bed with a fake tooth and playdoh practicing anatomy. HOURS. MONTHS. I was determined that if I didn't pass the test, it wasn't because I didn't know how to do fillings. I had done EVERYTHING in my power to pass and it was out of my hands. Don't get me wrong, I had studied and practiced for the first three times I took the test as well, but this time I kicked it up a notch to go from "good" to "GREAT."
One night before taking the test my final time, I had an "a-ha!" moment and that art piece finally CLICKED for me. It all made sense. The angles of the margins, the anatomy of the teeth, the way I needed to hold my instrument to make it look like how I finally could properly see it in my mind… it finally clicked and it was like the heavens opened up and angels sang around me!! I wondered if this is how it is for some clinicians where this piece DOES come naturally- the ones in the clinic who pick up their clinical skills quickly and what appears to be so effortlessly. And now here I was thinking that all of this restorative stuff is actually kind of fun, and not just struggily?! I knew right then and there I was going to not just pass, but I was going to kick that restorative test's butt! (Not that tests have butts, BUT(t) you get the point.)
I passed it on my FOURTH TRY, my final chance I was allowed to take it.
This final chance taking the test, I went into it calmly and felt at peace. I actually looked forward to it in a way because I was confident in myself and my abilities after all that preparation, not just praying I'd pass out of luck. And two weeks later (isn't that the longest two weeks of your life waiting to hear back your results?) when my phone buzzed that I had a new email from WREB, my heart stopped for a moment. I was out driving around with my sister and she was going on talking about something I couldn't even hear anymore after seeing those four letters pop up in my email. I couldn't wait, and yet, I couldn't open it at the same time!! Finally I opened it up and saw the best four letter word: PASS. Ahhhhhhhhh!!!!!!!!!!! I cried happy, victorious, relieved tears and felt so PROUD of myself. Genuine pride in myself that I'd worked so hard and been so dedicated to developing this "weakness" of myself into becoming a "strength." Proud that I didn't give up. Proud that I'd learned so much more by experiencing it THIS way instead of just passing it the first time. (by the way, 2/3 times I took it previously, I didn't pass by ONE point. If I had one single mark better, I would have passed! For some reason, that feels worse in a way than just totally bombing the test. Like.. Are you kidding me?! ONE POINT!!) THIS incredible feeling of accomplishment was worth all the heartache, frustration, sadness, and money I'd spent from before. This feeling was amazing. And I reached a place of acceptance beforehand of knowing if I hadn't passed, I would genuinely have been okay with that too. The journey itself was worth it and I'd already learned what I'd needed to learn, whether I passed this test or not.
To this day, passing that restorative test is one of my huge life-defining moments, right up there with delivering my two baby boys, and running a marathon. Like.. HUMUNGO MOMENT! My arch-nemesis test defeated by moi. I put SO MUCH into that test. And it paid off. I DID IT. I learned that day that I can do hard things. I can do ANYTHING. And YOU can too! I'm so glad I didn't let my FEAR of NOT PASSING get in the way of me trying. I could have dragged that guilt of 'what if?' my whole life, and instead I punched it in the face. (Again, not that tests have butts OR faces. And I promise I don't usually try to kick or punch so much stuff! Apparently I've still got some PTSD left behind from it--- I know you guys know what I'm talking about! ) I worked at an amazing pediatric office (Adventure Dental) putting that restorative license into action, which was quite a fun change of pace to my dental hygiene career
As humans we have a tendency to move AWAY from things that are uncomfortable, unfamiliar. We naturally stick to a place where it is safer, more secure, and predictable. I didn't HAVE to take this test again and put myself through torture, but I CRAVED seeing what I COULD do, seeing what I WAS able to accomplish, discovering what I was capable of. And when you get that burning desire inside you to try something different, and you're scared because you don't know what you're doing, DO IT! Go for it! Seriously! You have five seconds to take action following an idea before you'll talk yourself out of doing it. So whatever you just thought of right now as you read this, it is worth exploring, it is worth trying.
Why are we so afraid to try? Often we aren't afraid to try, but we're afraid to FAIL. I firmly believe this quote by R. Buckminster Fuller that "There is no such thing as failure, just outcomes." It's true. And the less afraid I am of "failure" whether it is in the form of passing a dental test or quitting an addiction, or answering something calling me from inside, and instead I choose to get CURIOUS and dig in and dive deeper, the more I learn, grow, and understand myself, life, and our world in general.
I'll leave you with a couple more inspirational quotes to lovingly pull you out of your comfort zone:
"Lean into the discomfort of the work." -Brene Brown
"If it excites you and scares you at the same time, it might be a good thing to try." -Seth Godin
What are some ways you've felt you've turned your "failures" into "successes?" I'd love to hear you share your experiences!
Nancy Huckvale, RDH graduated from the Utah College of Dental Hygiene in 2010. Since then, she’s practiced dental hygiene in Utah, Washington, and Oregon. Currently, she’s living in Logan, UT working at Logan Peak Dental and LOVING life. Nancy genuinely loves people, learning, connection, ducks, running, zumba/dancing, nature, trying new things to learn about different cultures, and kids. For any questions, she can be contacted by email: Nanhuck@Live.com.
Winners of Our Recent Giveaways for the XP Sharpen-Free Technology
We want to thank all of those who entered our recent giveaways for the American Eagle XP Sharpen-Free Instruments. Please email us at hygieneedge@gmail.com to claim your prize.
Blackjack- Trish O'H.
Barnhart 5-6 Kellie P.
M23 Jessica M.
Your Choice of a BH 5-6, Blackjack or M23 Crystal B.
